

Two Worlds of Medicine 🌍/📖
The stark contrast between textbook medicine and medicine in the real world.

Hello, and welcome to Reflections, a newsletter on health, wealth and family. I'm Sanuj, an internal medicine physician. If you're new here, you can learn more about Reflections in the about page. And if you think this newsletter is for you, hit the subscribe button to get regular updates.
Harrison’s Principles of Internal Medicine is one of the ‘go to’ reference textbooks for any physician or internist. Every disease in the book contains a discussion on its etiology, pathogenesis, clinical features, and eventually its management. Malaria has a treatment and travel prophylaxis algorithm. If a patient has end stage kidney disease, advise dialysis and a kidney transplant. If a patient has a treatable cancer, perform surgery, extract the tumour, add a pinch of radiation, chemotherapy or both. Throughout medical school and beyond, I've delved into multiple clinical guidelines for various diseases, all of which are a part of textbook medicine or will be in a future print. However, as any seasoned physician can attest, the reality of practicing medicine often diverges significantly from the idealized scenarios presented in textbooks.

Why is there a difference between real world medicine and textbook medicine?
Guidelines, as the name suggests, guides us to administer the most appropriate treatment based on the best available research evidence. To make a guideline is no easy task. It takes many days, if not months, of discussions among scientists, researchers and clinicians, carefully contemplating the advantages and disadvantages of each step in the guideline after a thorough review of available evidence. Diagnostic and treatment guidelines suggest the best course of action to tackle a disease for an optimal outcome. However, it is equally difficult to implement those guidelines universally.
One of the most striking differences between textbook medicine and real-world medicine is the complexity and variability of patient presentations. In textbooks, diseases are often described in neatly delineated categories, each with its own set of defining features and treatment algorithms. However, in clinical practice, patients frequently present with symptoms that don't fit neatly into these categories, or they may have coexisting medical conditions that complicate diagnosis and management. Here lies the difference between the two worlds of medicine, one from the books that educates us and the other from real world experiences and patients that actually teach us how inadequate all these books and guidelines are.
The two worlds of medicine are also divided by privilege. Privilege is not limited to finances alone. The privilege in healthcare is threefold:
Adequate finances - this includes health insurance coverage too.
Access to healthcare - transport, such as an ambulance, and the time taken to arrive at the healthcare centre (lesser the better) including the availability of adequate roads that reach there from all corners.
Availability of healthcare resources - the healthcare facility should have the necessary resources to diagnose and treat the underlying patient condition. This includes technology, specialized labs, and trained healthcare staff.
Textbooks often describe idealized healthcare settings with access to state-of-the-art technology, well-staffed facilities, and ample resources. However, in reality, many healthcare systems face constraints such as budgetary limitations, staffing shortages, and disparities in access to care. Difficult decisions may have to be made regarding resource allocation. These decisions can have ethical implications and may cause moral dilemmas.
The PET CT Conundrum
As part of the complete diagnosis and staging of many cancers, a positron emission tomography (PET) scan is advised to assess for spread of the disease. This PET scan machine per patient ratio is inadequate in many countries and even absent in many.
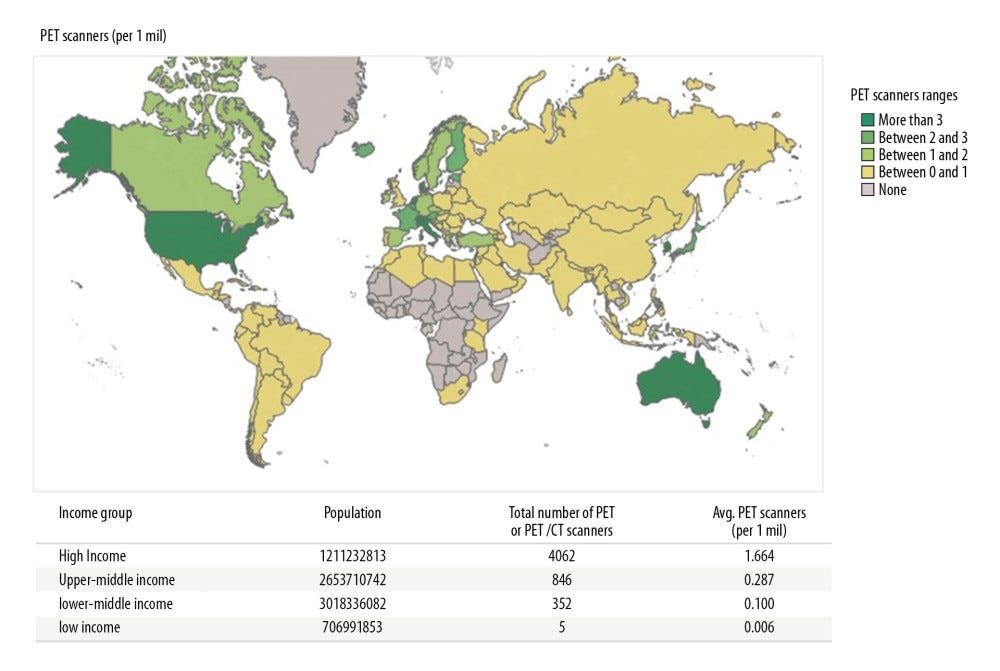
India and China, with its massive population, have lesser PET scan machines for a given number of people, than Australia, New Zealand or Japan for the same number of people. Many countries in the African and Asian continents have never had a PET scan machine in their land yet. This is an inequity in healthcare facilities. But the guideline in the medical textbook says that the cancer has to be staged based on the extent of spread shown by the PET scan. Now, imagine if I were in a country without a PET scan or the nearest PET scan machine is more than 500 kilometres away. How can I follow this guideline? Do I have to resort to less than standard facilities for my patient because of lack of resources? Or should I ask my patient to go to another state?
That's just one part of the dilemma. Now, say the machine is available nearby or in the hospital I work in. The cost of a PET CT scan is anywhere between ₹20,000- ₹35,000 (241-422 USD). If the patient is a daily wage labourer with cancer who earns less than ₹10,000 (120 USD) per month, what are my options? The guideline still says do the PET CT. It does not mention what to do if finances are limited. Cost, access and availability of diagnostic and management facilities are not part of treatment guidelines. The book is only partially helpful in the real world.
Resource Limitation in the case of a stroke
A new onset stroke is an emergency. A patient with an acute stroke has a chance for reversal, under appropriate conditions, if they present within 4.5 hours to a facility that has a competent neurology and radiology team. A CT scan of the head is needed to rule out a bleed in the brain. The treatment for a bleed related stroke is entirely different from a stroke caused by a block in the blood vessel to the brain. Stroke victims in villages are taken to quacks first, where no relief is found, and they arrive late at a hospital that has facilities for diagnosing and treating stroke. Even, if they recognize a stroke in the first 4.5 hours, the nearest hospital with a stroke management team is more than 4.5 hours away. Textbooks and guidelines do not account for this lacuna in the real world.
The Real World of Medicine
The medicine we read in our textbooks or from articles that suggest standard guidelines is only applicable to those with access to medical care. The vast majority of patients worldwide are not treated based on standard guidelines. The reasons for this are manifold as outlined above. The textbook world of medicine is filled with algorithms. Diagnosis is based on these algorithms. More like pattern recognition. I see a set of presentations, do necessary investigations and then boom - here's the diagnosis.
This is obviously necessary to treat the illness adequately. But the real world of medicine is not limited to treating a disease alone. Instead, it takes a step further into holistic care of the patient and not the disease per se. Real world medicine deals with tackling human emotions, following ethical treatment, and addressing patient and bystander concerns. Algorithms come second. A quote from the movie Patch Adams, portrayed by the iconic Robin Williams, exemplifies my viewpoint.
You treat a disease, you win, you lose. You treat a person, I guarantee you, you’ll win, no matter what the outcome.
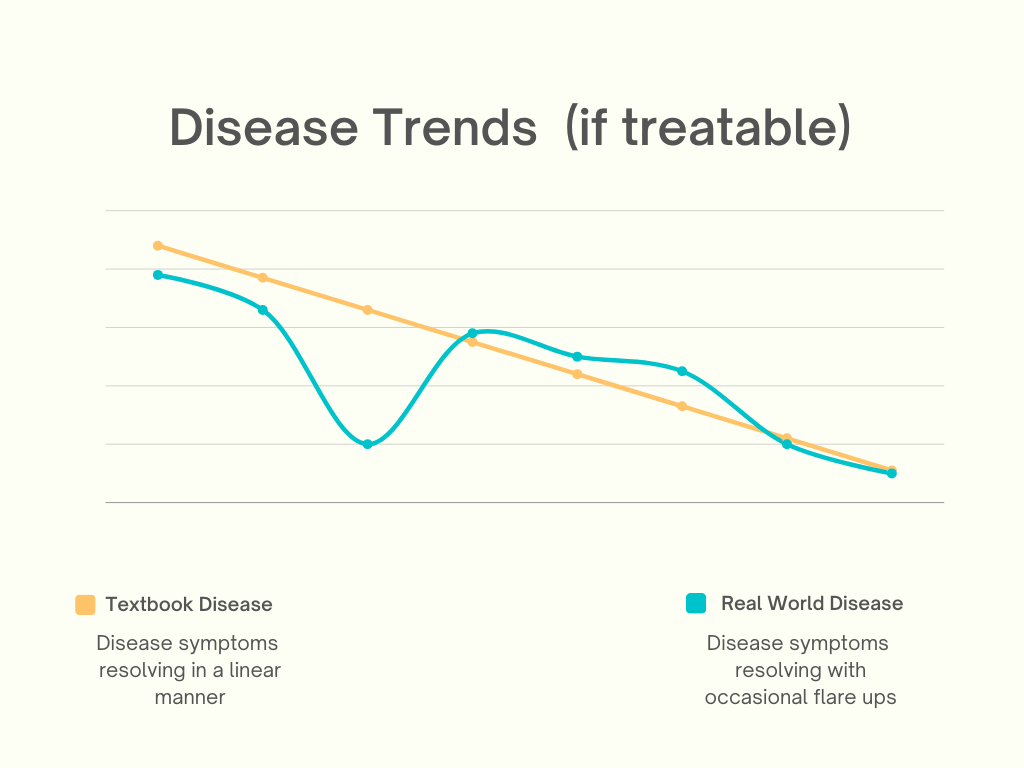
Illnesses rarely follow a linear path to recovery. The natural course of any disease is filled with crests and troughs. The disease may resolve with occasional flares followed by remissions. Or the disease may deviate from the original trajectory due to a new complication. A patient in the intensive care unit on a ventilator treated for an autoimmune disease like SLE (systematic lupus erythematosus) may, unfortunately, go on to develop ventilator associated pneumonia, despite the best possible care. Our textbooks don’t prepare us for this tangential deviation from the presenting condition. The new complication adds to both patient, hospital and caretaker burden.
Acknowledging the two worlds
Textbook medicine tends to emphasize evidence-based guidelines and standardized protocols for patient care. While these guidelines are invaluable tools for informing clinical decision-making, they may not always account for the nuances of individual patient circumstances. In the real world, patients often have unique medical histories, preferences, and socioeconomic factors that can influence their treatment outcomes. For instance, a guideline-recommended medication may not be suitable for a patient due to allergies, intolerances, or financial constraints. In these situations, physicians must tailor their approach to care, taking into account the patient's individual needs and circumstances.
While textbooks serve as indispensable resources for medical education and training, they only provide a partial glimpse into the complex and dynamic world of real-world medicine. The practice of medicine is characterized by uncertainty, variability, and nuance, requiring healthcare providers to adapt their approach to care to meet the unique needs of each patient.
The two contrasting worlds of medicine reflect health inequity and it is, unfortunately, here to stay. Despite our best efforts, we cannot overcome the randomness, diversity and social circumstances of patients and their clinical presentation. Following guidelines are still the best way to approach a disease, but beyond that we may have to improvise and adapt based on the patient and the resources available within our grasp. It sometimes requires deviating from strict textbook protocols to provide personalized care.
Great insights - there's a lot of economics involved in what you're discussing. It also reminds me of a comment I heard by a CEO, who basically stated that we often think the most skilled managers and executives are in the top firms in the world, but if these managers were put to run a company or factory in a place that encounters many unforeseeable issues such as rolling electric blackouts, unreliable transport etc, they'd fail within a quarter. Results depend on how well oiled the machine is and if everything is perfect, we can do a lot. But we also need guidelines for situations that are far from perfect.
Another variable in patient care is insurance. Health insurance companies are increasingly involved in decisions about diagnosis and treatment. As an example, my daughter’s oncologist ordered a PET scan only to have her insurance company representative, a pharmacist, say she couldn’t have it. It was wrong to deny my daughter’s physician access to the information she needed to treat her patient.
This is just one example but the problem is getting worse. Something needs to change.